

Do I Just Need a Routine Cleaning or Something More?
“I just need a cleaning.” We hear this all the time. And honestly, it makes sense. Your teeth look fine, nothing hurts. You brush. You floss… mostly. From your point of view, everything seems pretty normal. The tricky part is that gum health isn’t something you can see in the mirror. Dentists and hygienists are […]
Read more

Why Following Up After Immediate Dentures Matters: A Real Patient’s Worst-Case Scenario
When “Immediate” Doesn’t Mean “Done” There are few things more intimidating than the prospect of extracting your teeth and getting a denture; it’s a big decision, emotionally, physically and financially. That’s why immediate dentures can feel like such a lifesaver! We place them the same day as your extractions, so you don’t have to leave […]
Read more

Tooth Loss Triggers Bone Loss: The Clock Is Ticking
As dentists, we often talk about the importance of replacing missing teeth, but there’s a hidden reason behind that advice that goes beyond chewing, smiling, or even avoiding that “sunken” look. It’s something happening under the surface: bone loss. What You Don’t See Will Cost YouMost people think losing a tooth is the end of […]
Read more

“Kiss Me, I’m Cavity-Free”
How Your Oral Hygiene Affects Your Loved Ones We all know that love is contagious, but did you know cavities can be too? That’s right. Your oral hygiene doesn’t just affect your own smile, it can actually impact the oral health of the people you love most, because oral bacteria gets passed from one person […]
Read more
Leisure Suits & Dental Fit: Choosing High-Quality Dentures for Comfort and Function
Acid-washed jeans, polyester leisure suits, plastic ‘jelly’ shoes, and denim cargo shorts— all fashion trends that have gone into extinction, much to my relief before the era of smartphones and social media. As a result, you won’t find photographic evidence of me in those outdated fashions of yesteryear, unless you’re privy to my mother’s living […]
Read more
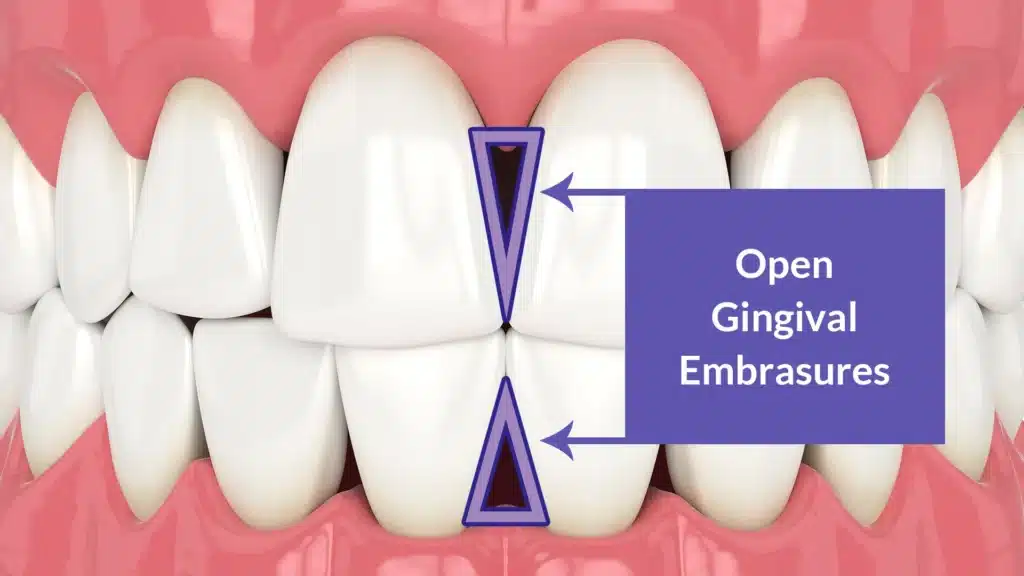
Restoring Black Triangles
In my latest feature in LA Metro Magazine’s “PROS WHO KNOW”, I talked about a common dental frustration that affects up to 67% of people over the age of 20: black triangles—the small, dark spaces that appear between teeth due to gum recession or bone loss. Many patients don’t even notice them until they suddenly […]
Read more

Decoding Periodontal Health with Saliva Testing
In my recent feature in LA Metro Magazine under the “PROS WHO KNOW” section, I addressed a common frustration in dental health: periodontal bone loss despite diligent oral care. This phenomenon, often experienced by patients who actually take really good care of their teeth, can be attributed to gum disease and its associated complications. Based […]
Read more

Are Bleeding Gums Normal?
Are bleeding gums normal? The short answer is no, bleeding gums are not generally normal. Are Bleeding Gums Common? Yes, they’re way more common than you think. Let’s face it, we all know flossing doesn’t always make the cut in our daily routines. But here’s the deal: your gums are just as important as your […]
Read more

Why Implant Supported Dentures Could Be the Answer
It’s always kind of fun to start punching something into Google and see what’s suggested, even more so when you are legit scanning for research information on a subject that’s close to heart. As a dentist, I don’t tend to google dentistry questions, 80’s wrestling is more my style, but I do get that the […]
Read more

Does Brushing Harder Clean Your Teeth Better?
Sometimes I see Lady Macbeth in my office. I’m sure you’re familiar with Shakespeare’s play, we all had to read it and maybe even perform it in high school, right? You know, the one that opens with the witches chanting about “toil and trouble”, finds Macbeth pondering, “Is this a dagger which I see before […]
Read more